
Licensed professionals can receive the latest Listerine clinical information and patient resources.

A LANDMARK META-ANALYSIS DEMONSTRATES HOW TO TREAT A GLOBAL ORAL HEALTH PROBLEM. AND IT STARTS WITH YOU.
As a dentist, you know that oral disease is widespread. But you may be surprised by the severity of the situation.
Bold Facts:
- A recent study revealed that untreated oral disease affects approximately 3.9 billion people globally. That’s more than half the planet’s total population1,2
- 90% of the world has some degree of chronic gingivitis3
- In most industrialized countries, oral disease is the 4th most expensive disease to treat4
As the makers of LISTERINE®, we want to share with you some bold insights from a landmark meta-analysis that sheds light on how some of the products available to you and your patients can play a leading role in addressing this global health issue.
As you know, a healthy mouth requires controlling biofilms.5-9 Plaque control is fundamental to achieving oral health.10,11 And, while the standard recommendation for at-home oral care focuses on mechanical methods, brushing and flossing aren’t enough.10,11 In fact, research shows that brushing and flossing only removes approximately 42% of plaque*.12
Removing plaque from the tooth surface is crucial. But, the tooth surface is only 25% of the total area of the mouth exposed to bacteria.13 Other areas in the mouth can act as reservoirs for bacteria that can then re-colonize bacteria on teeth following dental prophylaxis or cleaning treatment.14
The good news is, a landmark meta-analysis has concluded that LISTERINE® Antiseptic can provide a benefit beyond mechanical oral hygiene alone in preventing and reducing plaque accumulation and gingivitis.15
The meta-analysis evaluated these studies with a focus on outcomes applicable to clinical practice. It reviewed randomized, observer-blind, placebo-controlled, published and unpublished clinical studies assessing the effect of an essential oil-containing mouthrinse (MMEO) vs mechanical methods in subjects with mild-to-moderate plaque and gingivitis. The magnitude of the pooled study is extraordinary15:

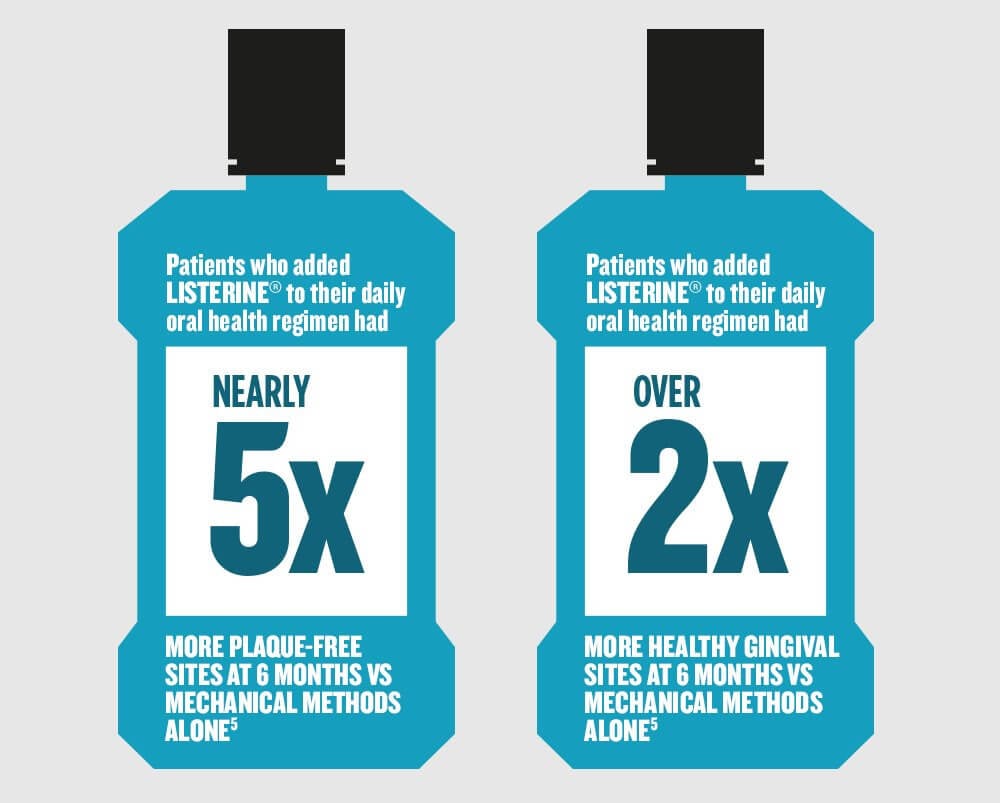
The bold results: Unequivocal proof that daily use of an essential oil (EO) mouthrinse like LISTERINE® Antiseptic, along with mechanical oral hygiene, provides greater prevention of gingivitis and plaque buildup than mechanical oral hygiene alone.
Specifically, at 6 months, MMEO subjects had nearly 5 times more plaque-free sites vs mechanical method subjects, and over 2 times more healthy gingival sites vs mechanical methods as well.15
So what does this mean for your practice?
It means that when your patients use an EO mouthrinse like LISTERINE® Antiseptic, you can be confident that it is:
- Reaching even the hardest-to-reach areas of their mouth
- Killing bacteria down the to the bottom layer
- Helping maintain the oral microflora at levels compatible with a healthy mouth
All of which can provide a clinically significant benefit to the patient.7,9
Despite the availability of preventive measures, untreated oral disease remains a significant global burden.1 And, while you can’t treat the entire world, you can suggest to patients that adding LISTERINE® Antiseptic to brushing and flossing can provide greater prevention of gingivitis and plaque buildup than mechanical methods alone.
And that’s a bold start.
We hope you found this article of value.
CLINICAL INFORMATION ABOUT LISTERINE® ANTISEPTIC.
Discover a wealth of evidence about the benefits of LISTERINE® Antiseptic mouthrinse.

WHAT’S BOLDER THAN BETTER ORAL HEALTH FOR ALL?
Proof that it’s possible.
BOLD INSIGHTS FROM A MILESTONE INVESTIGATION. Footnotes
*Depending on index used.
References: 1. Marcenes W, Kassebaum NJ, Bernabe E, et al. Global burden of oral conditions in 1990-2010: a systematic analysis. J Dent Res. 2013;92(7):592-597. 2. Census population clock. https://www.census.gov/popclock/. Accessed May 2, 2016. 3. Coventry J, Griffiths G, Scully C, Tonetti M. Periodontal disease. BMJ. 2000;321(7252):36-39. 4. Oral health. Fact sheet No 318. April 2012. World Health Organization Web site. Accessed April 17, 2015. 5. Marsh PD. Are dental diseases examples of ecological catastrophes? Microbiology. 2003;149:279-294. 6. Do T, Devine D, Marsh P. Oral biofilms: molecular analysis, challenges, and future prospects in dental diagnostics. Clinical, Cosmetic, and Investigational Dentistry. 2013;5:11-19. 7. Gurenlian JR. The role of dental plaque biofilm in oral health. J Dent Hygiene. Suppl:4-11. 8. Marsh PD. Dental plaque as a biofilm: The significance of pH in health and caries. Compendium. March 2009;30(2):76-87. 9. Marsh PD. Contemporary perspective on plaque control. Brit Dent J. 2012;212(12):601-606. 10. Gunsolley JC. A meta-analysis of six-month studies of antiplaque and antigingivitis agents. JADA. 2006;137:1649-1657. 11. Gunsolley JC. Clinical efficacy of antimicrobial mouthrinses. J Dent. 2010;38(I):S6-S10. 12. Slot DE, Wiggelinkhuizen L, Rosema NAM, et al. The efficacy of manual toothbrushes following a brushing exercise: a systematic review. Int J Dent Hygiene. 2012;10:187-197. 13. Kerr WJS, Kelly J, Geddes DAM. The areas of various surfaces in the human mouth from nine years to adulthood. J Dent Res. 1991;70(12):1528-1530 14. Boyle P, Koechlin A, Autier P. Mouthwash use and the prevention of plaque, gingivitis and caries. Oral Dis. 2014;20(suppl 1):1-68. 15. Araujo M, Charles C, Weinstein R, et al. Meta-analysis of the effect of an essential oil-containing mouthrinse on gingivitis and plaque. J Am Dent Assoc. 2015;146(8):610-622 and/or post hoc analyses of data.
All Fields required, unless otherwise indicated
Personal Information
Step 1
Will be used as your user name
By submitting your information above, you agree that the information you provide will be governed by our site's Privacy Policy.